 In contact with the wound exudate, the TLC-Ag matrix forms a gel, creating a moist environment that promotes wound healing.
In contact with the wound exudate, the TLC-Ag matrix forms a gel, creating a moist environment that promotes wound healing.
Simultaneously, the hydro-desloughing, polyabsorbent polyacrylate fibres absorb excess exudate, forming a gel. These hydro-desloughing fibres bind to the sloughy residues, absorbing and draining them in order to facilitate autolytic debridement.
This binding and drainage of slough by the hydro-desloughing structure of UrgoClean Ag combined with its Silver healing matrix (TLC-Ag) thereby promotes the desloughing phase of sloughy wounds, and aids management of minor bleeding (particularly after mechanical or surgical debridement).
In addition, the Ag+ ions give UrgoClean Ag an antibacterial activity that could help reduce the local bacterial load. The Ag+ ion has broad-spectrum antimicrobial activity, and is particularly effective against Staphylococcus aureus, MRSA, Streptococcus pyogenes and Pseudomonas aeruginosa (pyocyanic bacillus), the microorganisms most commonly implicated in infected wounds. The antibacterial activity of the dressing helps reduce odour caused by microorganisms present in the wound. UrgoClean Ag reduces the bacterial population of the biofilm within 24 hours and for 7 days (tested in vitro on S.aureus and P.aeruginosa).

The dressing is practical for patients, because it can be removed in one piece due to the tensile strength of the hydro-desloughing fibres. The gel formed does not stick to the wound, making it easy to remove the dressing, painlessly or with only minor pain and with little or no damage to healed tissue.
- Broad spectrum antibacterial activity, including MRSA (1)
- 99.9% removal of biofilms after 1 day (2)
- Pain-free dressing changes (3,4,5,6)
- Well-tolerated (7)
- Moist wound-healing (3,8)
- Clinically proven in a Randomised Controlled Trial (7)
 Contraindications:
Contraindications:
- Known sensitivity to silver.
- UrgoClean Ag is not suitable for use as a surgical sponge for heavily bleeding wounds.
- Do not combine UrgoClean Ag with hydrogen peroxide or organic mercury or hexamidine antiseptics.
- Do not leave the dressing in place on the patient during Magnetic Resonance Imaging exams (MRI scan).
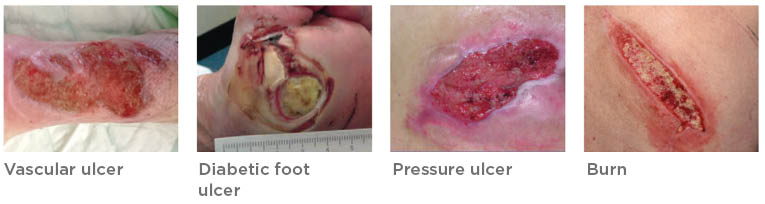
Indications:
- Non to low exuding wounds, infected or at risk of infection
- Can be combined with an absorbent layer
- Can be used in cavity wounds

- Wound preparation:
- Clean the wound with normal saline. In the event of prior use of an antiseptic (except contraindicated antiseptics), rinse the wound carefully with normal saline before applying the dressing.
- The use of UrgoClean Ag does not dispense with the need for associated mechanical debridement when required.
- During desloughing, the wound may appear to get larger due to gradual elimination of slough.
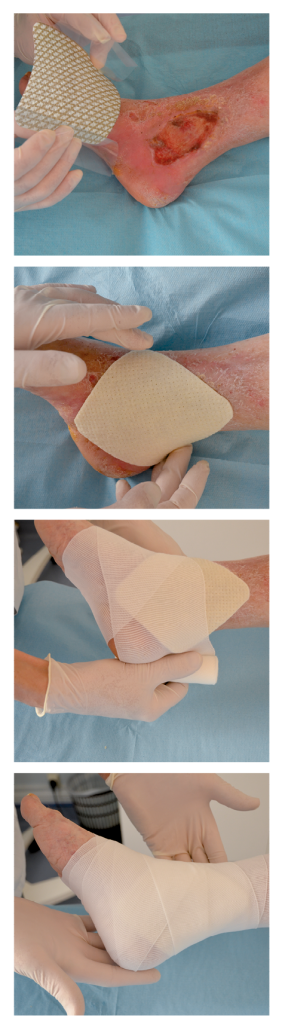
- Dressing application:
- Remove the protective tabs.
- Apply with the micro-adherent side of UrgoClean Ag in contact with the wound and its edges.
UrgoClean Ag can be cut using sterile scissors to adjust the dressing size to fit the wound if necessary.
- If necessary, cover UrgoClean Ag with a secondary dressing suitable for the wound location and level of exudate.
- Secure in place with a suitable bandage or tape.
- Apply a compression bandage where prescribed.
- Dressing changes:
UrgoClean Ag should be changed every 1 to 2 days during the wound desloughing phase, then as often as required (up to 7 days) depending on the exudate volume and the clinical condition of the wound. The maximum treatment duration with UrgoClean Ag is 1 month.
Precautions for use:
- Treatment with UrgoClean Ag should be performed under medical supervision.
- The use of this dressing does not dispense with the need for appropriate systemic antibacterial treatment for infected wounds, in accordance with local treatment protocols.
- The silver-impregnated micro-adherent healing matrix (TLC-Ag) in UrgoClean Ag sticks to latex surgical gloves. It is therefore recommended that the dressing be handled carefully, avoiding any contact with the micro-adherent side, or using sterile tongs.
- The concomitant use of other local treatments is not recommended.
- Avoid contact with electrodes or conductive gels during electronic measurements, such as EEG or ECG recordings.
- Clinicians and healthcare professionals must take into account the fact that data concerning the prolonged and repeated use of a silver dressing, particularly in children and newborn babies, is not very extensively documented.
- In the absence of specific clinical data, the use of the UrgoClean Ag dressing during pregnancy or breastfeeding or in newborn or premature babies is not recommended.
- UrgoClean Ag must not be used during hyperbaric oxygen chamber therapy without an oxygen mask (risk of combustion due to the presence of fat). This contraindication does not apply for hyperbaric oxygen chamber therapy with an oxygen mask if the oxygen concentration inside the chamber is less than 25% and if UrgoClean Ag is not applied on the area over which the mask is placed.
- Sterile individual packaging, for single use. Reuse of a single-use dressing can lead to risks of infection.
- Check that the sterility protector is intact before use. Do not use if the packaging is damaged.
- Do not re-sterilise.
- For disposal, refer to the existing protocol. Discard any unused parts of the dressing.
Method of use:
- Add a secondary dressing
- Secure with a retention bandage (K-Band, K-Lite)
- Can be left in place for up to 7 day